As you know from our blog post on rotator cuff surgery, we used to work alongside a shoulder surgeon. What we didn’t mention is that we actually worked with two surgeons. The second surgeon specialized in hip and knee surgeries.
This also translated to significant experience treating post-operative knee replacements, hip replacements, ligament reconstructions, knee scopes, and meniscus repairs. This blog post will cover the last two: knee scopes and meniscus repairs.
Thus, the purpose of this blog is to try and clarify the ins and outs of a knee scope/meniscus repair. There’s LOTS to know, and if you’re going to go through any surgery, it’s nice to feel prepared!
Aside: We will use the same headings in this post as we did in the rotator cuff surgery post. We’ll try to stick with the same format so that it’s easier to navigate. Some things might look similar, as some advice is “surgery” related, and less specific to the type of surgery.
How do I know if I even need a knee scope/meniscus repair?
Typically, to qualify for a knee scope or meniscus repair, the following statements are true:
- You have significant knee pain that is greatly limiting your ability to complete your activities of daily living (i.e. walk, sleep, work)
- You have imaging results (i.e. an MRI) that show meniscus or knee joint damage
- You have tried to reduce your pain and improve your function through virtually every other conservative option, including a significant bout of physical therapy
- Conservative options include, but are not limited to: physiotherapy, massage therapy, chiropractic care, acupuncture, and injections
Now for the science. Some people might find this science hard to swallow, so we’ll be sure to back it up with scientific proof. We’ll then go on to state the couple more statements that should be true if you intend on undergoing a knee scope/meniscus surgery.
To limit the plethora of different research papers we could include to show the most effective treatment option for degenerative knee arthritis and meniscal tears, we’ll focus on just one.
Here’s the reference:
Here’s what it says:
The authors of this research paper did the following for us:
- Combined all of the research on the treatment effectiveness of a knee scope (arthroscopic surgery) for knee arthritis and meniscal tears (degenerative changes)
- Combined all of the research on the treatment effectiveness of conservative management (i.e. physiotherapy) for knee arthritis and meniscal tears (degenerative changes)
This is their conclusion:
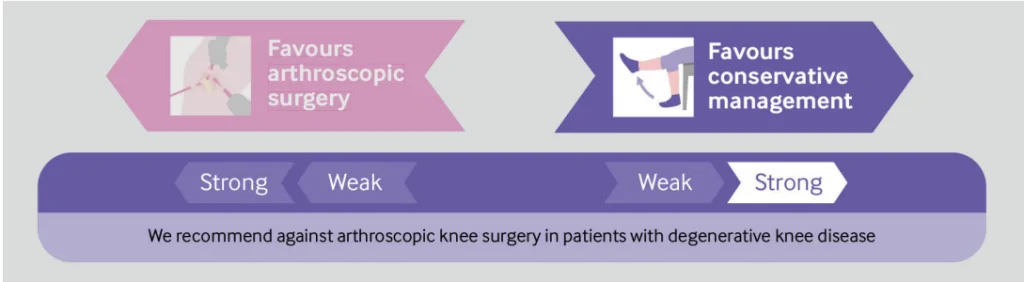
If you’re interested in more than just 1 reference, go read these clinical practice guidelines. They include more than 30 references, including multiple systematic reviews (which are the highest level of evidence). You can find it here, for free.
In short, this is what the research says: do not have a knee scope surgery for degenerative knee/meniscus changes. Do physiotherapy instead.
If you think surgery is still the right option, consider these statements in addition to the ones listed above. As they should also be true:
- You remember the moment you injured your knee – it usually happens during an accident or trauma in which you will remember feeling pain at a specific point in time
- You have significant objective locking of your knee that gives you pain and greatly limits your ability to function (it gets physically stuck)(and this locking is persistent, severe, and frequent)
- There is a clear evidence of a meniscus injury/tear, that is not due to “degenerative changes”
Do I have to do pre-operative physiotherapy?
In short, yes, you should. It helps in the following ways:
- Helps you understand what to expect with surgery and postoperatively (just like this blog post should!)
- Helps strengthen muscles to their maximum potential (not just knee muscles, but also ankle, hip, and core muscles)
- Improves your range of motion to help limit stiffness in all associated joints
- Can help you gather baseline measurements to track your progress post-op
- It will allow you to skip the surgery part altogether (see above!)
What else should I do before I get a knee scope/meniscus surgery?
- Understand what you’re getting yourself into
- Eat well and take steps to improve your overall health (i.e. quit smoking)
- Get any equipment your surgeon recommends (i.e. compression sleeve, or crutches)
- Organize assistance for after surgery (in some cases you must use crutches, or you won’t be able to drive)
How is a knee scope or meniscus surgery performed?
Every surgeon has their individual preferences, however, most surgeons do meniscus surgeries arthroscopically (arthroscopic is where “scope” comes from). Arthroscopic means that the surgeon will use a tiny camera called an arthroscope. The arthroscope is inserted into your knee joint via a fairly small incision. The tools required to fix your meniscus/complaints are inserted through additional small incisions. Therefore, you’ll likely only have a few (2-3) small incisions around your knee!
Typically, when only the term “knee scope” is used, the surgeon is using a small tool to perform a ‘debridement’ of the knee joint surfaces. Debridement essentially means that the surgeon is ‘cleaning up’ the degenerative/damaged tissue within the knee (like small pieces of bone called “osteophytes”).
Even though a meniscal surgery is also technically a “knee scope”, usually people are more specific and include the word “meniscal” somewhere. When doing a meniscal surgery, the surgeon has a couple of options. At their discretion, they will perform a meniscus repair, in which they will stitch the meniscus tear back together.
Or they will perform a “meniscectomy”, in which they will remove a section (“partial meniscectomy”) or all (“full meniscectomy”) of your meniscus (and no, they don’t replace it with anything).
Psst. If you want to know more about knee anatomy, check out our post here.
Disclaimer:
Before we get into the next part of this blog post, it is important to note that everything in this blog post is for information purposes only. This blog post is not intended to be strict medical advice. As previously mentioned, everyone is an individual, and therefore, individual variances do occur. It is important to consult your physiotherapist, surgeon, or doctor for the most applicable advice for you.
What does the typical rehabilitation process look like?
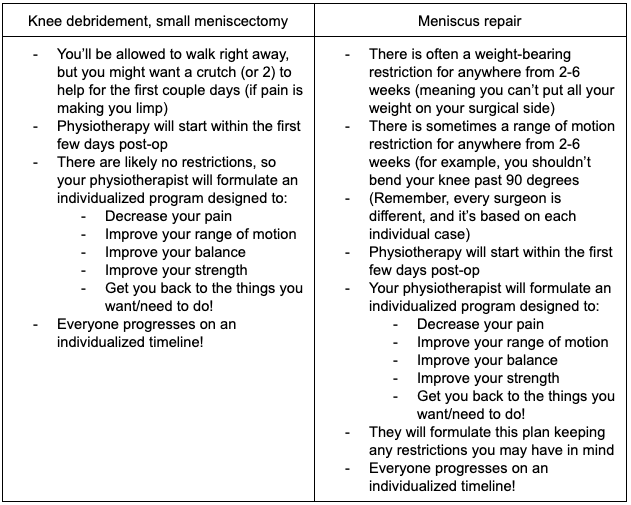
It depends on the exact procedure you had done. If you had a meniscus repair in which your meniscus was stitched back together, some surgeons will instruct you to have a period of non-weight bearing (meaning you can’t put weight on your surgical leg). Typically this is somewhere in the 2-6 week range.
That being said, studies are showing that this may be an out of date practice as research indicates that both early (accelerated) and restricted range of motion/weight bearing yield similar, good to excellent results. (VanderHave, K. L., Perkins, C., & Le, M. (2015). Weight-bearing versus non weight-bearing after meniscus repair. Sports Health, 7(5), 399-402.)
If you had a debridement or meniscectomy, you will most likely have no postoperative restrictions!
Therefore, post-operative care looks something like this (keeping in mind that every surgeon has their preferences):
How long does it take to heal after a knee scope/meniscus surgery?
In uncomplicated cases,- Surgical healing of your knee can take up to 8-12 weeks after surgery.
- Surgical healing does not always mean full function. It means the surgical sites and joint surfaces are likely physiologically healed.
- Full function is very individualized in the case of an arthroscopic knee injury and usually takes:
- Up to 6-12+ weeks for a knee debridement/small meniscectomy
- Up to 12-16+ weeks for a meniscus repair with post-operative restrictions
- Progressive, safe, and necessary functional strength training exercises will take months to appropriately complete.
- Additional note: in many cases, rehabilitation post-operatively is not just helping you heal from your surgery. You’ll also be rehabilitating the weeks-months of poor function you had before surgery!
- You may be off work a long time, depending on your job (for example: if you are on your feet constantly doing a lot of squatting and stair climbing, you will be off work much longer than someone with a desk job)
- Physiotherapy appointments will be necessary for at least a couple months. Yes, the frequency of appointments will decrease over time, but it will be important to stick with your physiotherapy appointments.
- If you have private insurance coverage, that’s great! But keep in mind, depending on how much you have, it is not uncommon to use all of it, and then some.
- If you don’t have private insurance coverage, rehabilitation costs will be expensive.
- Couple this with being off work and finances can be a significant added stress that many people do not consider!
- Be aware of the financial considerations associated with surgery.
What exercises are safe to do right away after a knee scope/meniscus surgery?
Again, this will depend on whether or not you have any post-surgical restrictions. If you have NO post-surgical restrictions, most exercises are considered safe. That being said, you’ll want to listen to your body, start slow, and progressively increase the load on your knee (We don’t recommend going for a run or jumping on a trampoline right after surgery!). Roughly, you will progress in this order with rehab:- Pain control
- Range of motion exercises
- Strength building exercises
- Motor control exercises
How much function and how little pain can I expect at the end of my rehabilitation?
Alas, the loaded question. Again, everyone is an individual, everyone heals differently, and therefore final pain and function is highly individualized. Here are some things we consider:- How much pain did you have before surgery, and how long did you have that pain?
- Again, these can be related. If you were in absolute agony for 3 years before surgery, there will be a lot of additional things to consider when trying to reduce pain post-operatively. Pain has biopsychosocial components. See this awesome blog post on pain for more information.
- If you tore your meniscus from a one-off accident, got assessed quickly, started pre-operative physiotherapy, and received surgery fairly quickly, there should be fewer things limiting your overall recovery.
- What are your goals?
- If your goal is to sprint and jump repetitively, your rehab will probably take longer than if your goal is to walk around and sit at your desk at work. Therefore, depending on your goals, your perception of your overall function will also change.
- That being said, set appropriate, attainable goals with your physiotherapist and work towards these goals!
- Operative and non-operative management of “degenerative” knee/meniscus changes have been shown to have the same long-term outcomes
- That being said, these outcomes are typically favorable!
What are the potential complications associated with a knee scope/meniscus surgery?
All steps will be taken to limit complications postoperatively, however, it’s important to understand the possibilities. Complications include:- Infection. It’s important to follow the hospital’s instructions on keeping your incisions clean, and free of debris. Change your bandages as instructed, and take good care of your wounds.
- Keep an eye out for:
- Ill-smelling, discolored discharge coming from your wounds.
- If you’re running a fever, have a significant increase in pain, swelling, or redness around the knee.
- Keep an eye out for:
- Deep vein thrombosis (DVT). This is a blood clot that can form in the blood vessels of your leg. Most commonly, in the calf muscle. Here’s what to look out for:
- If your calf (usually) or thigh is:
- Red, hot, and swollen
- Painful to touch, and painful with bending your ankle
- Throbbing or cramping
- These are the most common signs of a DVT. If you think you may have a DVT, go directly to the hospital. This is an emergency.
- If your calf (usually) or thigh is: